GM CASE WITH FEVER AND CHILLS
A 65 yr old male with fever and chills
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan. is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
A 65 years old male patient daily wage by occupation came to casuality with chief complaints of high grade fever ,chills and rigors, generalised weakness since 3 days
History of presenting illness::
Patient was apparently asymptomatic 2 yr back and then he developed high grade fever, intermittent, relieved on medication
patient had generalised weakness since 2 days
Patient is unable to daily activities since 1day
C/o giddiness since 1 day,
H/o fall (syncope)
H/o loss of consciousness ,SOB,chest pain, Palpations
Past History:
Patient is a known case of diabetes mellitus since 2 years
H/o left lower limb filariasis since 20 years
Personal history:
Apettite-normal
Diet- mixed
Bladder- normal
Bowel -regular
Family history:
No significant
General examination::
Patient is conscious,cohorent , cooperative well known with time, place, person
He is well built and moderately nourish
Pallor absent
No Peadal.edema
VITALS :
Temp : 102.6 f
Pulse rate-110 bpm
Blood pressure :160/80mmhg
Respiratory rate :25 cpm
Spo2 : 98%
SYSTEMIC EXAMINATION:
CVS :
Palpation:
No Cardiac murmurs
Respiratory system:
Inspection: chest shape normal,
Dyspnea: no
Palpation: trachea -central
Vesicular breath sounds
Abdominal examination:
Shape : scaphoid
Tenderness -no
Free fluid -no
Liver,spleen -not palpable
CNS: No focal neurological deficit
MANAGEMENT :
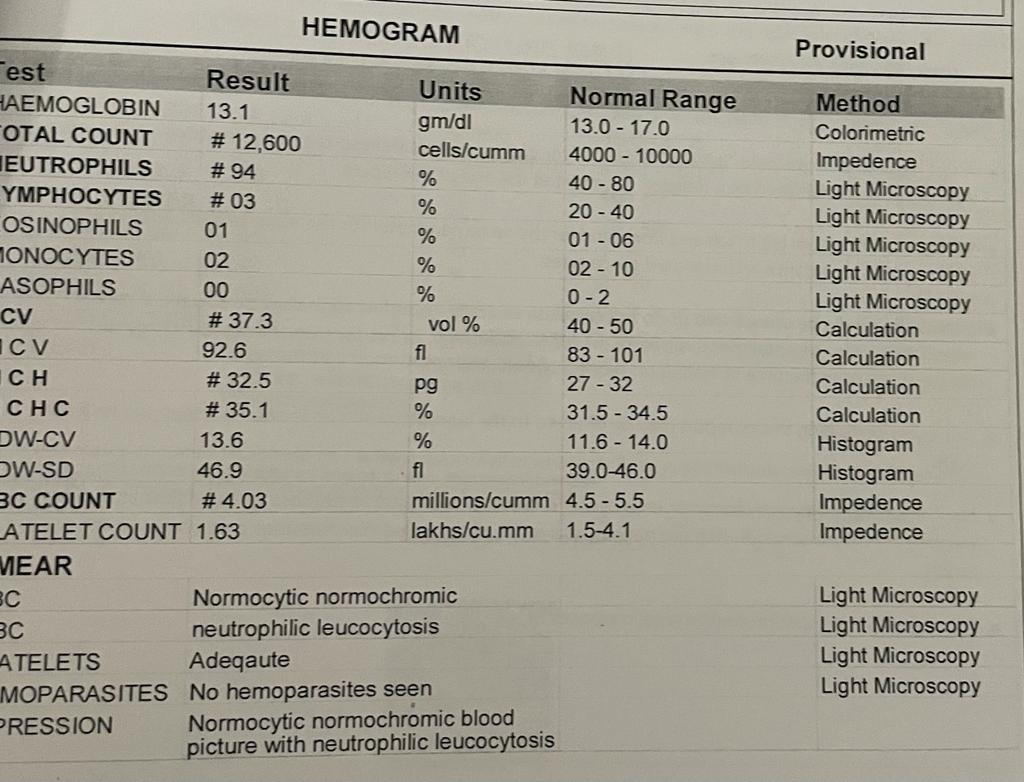
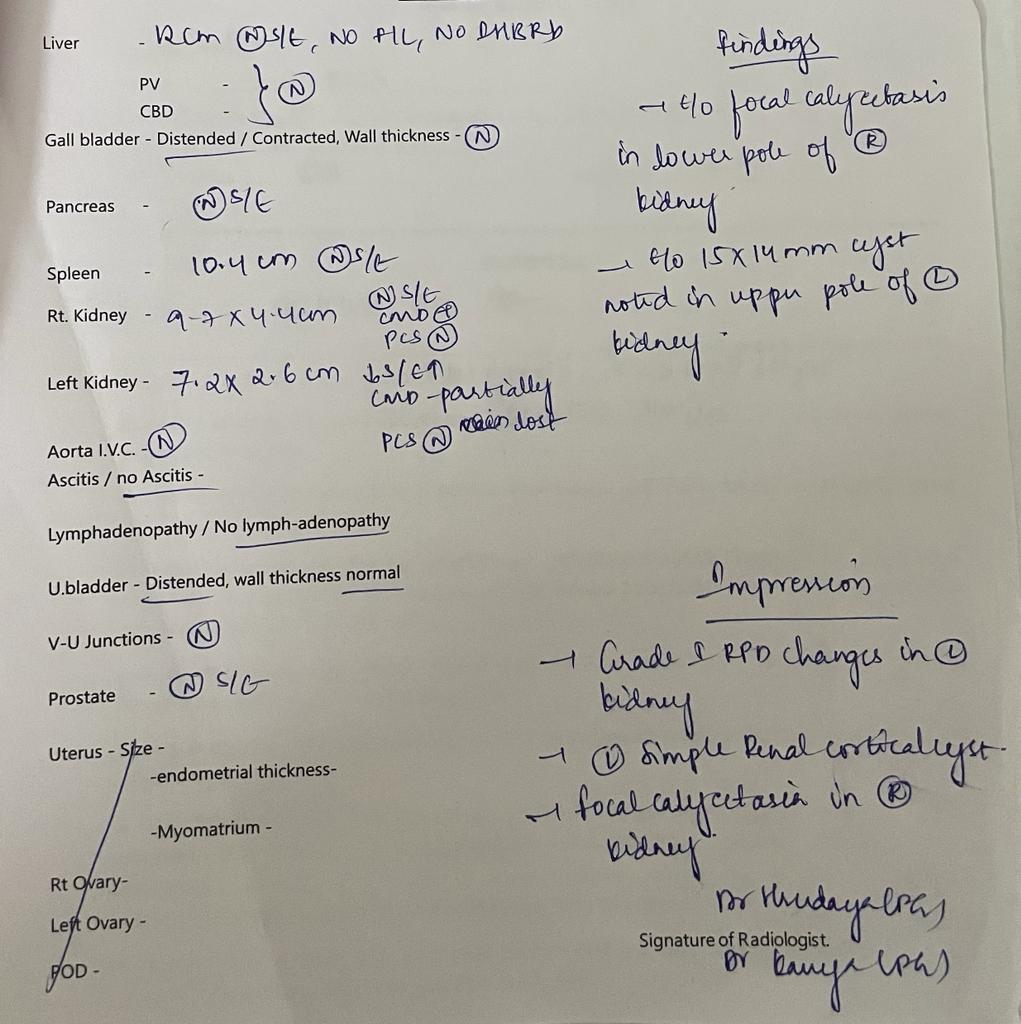
INVESTIGATIONS : Hemogram ,LFt ,serum electrolites,cbp,Grbs,Usg,ecg
Hemogram:











Comments
Post a Comment